Jaw Surgery in Washington, DC
Introduction
When a patient has a malocclusion that the orthodontist cannot correct with orthodontics alone, he/she may request that the patient see a surgeon to move the jaws into a more favorable position to eliminate the discrepancy between the upper and lower jaws. Orthognathic surgery (jaw surgery) is the name of the surgery that moves the jaws into a position so that the orthodontist can align the teeth into their optimal position. Patients may be referred to Dr. Baker when starting orthodontic therapy (it is obvious jaw surgery may be indicated), during orthodontic therapy (the orthodontist underestimated the difficulty of the patient’s malocclusion), or after braces are complete (the patient knew they would need surgery and decided to just see the surgeon when they were ready). Dr. Baker will review the advantages and disadvantages of both a surgical and nonsurgical approach so that each patient can make the best decision for them at the time. Patients also present to Dr. Baker directly with concerns of their facial form that may require orthognathic surgery to correct. Dr. Baker’s experience in both orthognathic and aesthetic surgery enable him to develop a plan that is both functional and aesthetic. The information in this booklet is written by Dr. Baker to inform his patients of the thought process and planning that are involved in orthognathic surgery.
Dr. Stephen Baker’s Credentials for Jaw Surgery
With training in dental, medical, oral and maxillofacial, plastic surgery, and craniofacial training, Dr. Baker is one of a select few surgeons in the world who has this type of experience in orthognathic surgery.
- Plastic surgery knowledge of facial aesthetics gives him insight in planning BOTH a functional and aesthetic result.
- Authored textbooks on jaw surgery, aesthetic facial surgery, and rhinoplasty International and national lecturer on jaw surgery
- Published many articles on jaw surgery
- Published many chapters on jaw surgery
- Leader in quality of life and outcomes studies in jaw surgery
- Pioneer of virtual surgical planning (computer aided surgical simulation) Pioneer of custom plates in orthognathic surgery
- Past President, American Society of Craniofacial Surgeons
- Past President, Northeastern Society of Plastic Surgeons
- American Society of Maxillofacial Surgeons Visiting Professor on jaw surgery
Ideal Candidates for Orthognatic Surgery
Any patient who has an underlying skeletal jaw malposition may be a candidate for jaw surgery. Typically, a patient who is considering jawsurgery is referred by their orthodontist when the orthodontist feels that the occlusion would be ideally corrected by moving the jaw bones into a more favorable relationship. When you are evaluated for surgery by Dr. Baker, he will not pressure you to undergo the surgery. He views his job as a physician to provide you with all the information you need to make the best decision for you. By educating his patients in the nature of surgery, he hopes to allow each patient to determine what is best for them in the moment but also in the future. The broad categories Dr. Baker evaluates for jaw surgery are described below.
Teenage patients are the most common group of patients Dr. Baker sees for evaluation for jaw surgery. Patients who have malpositioned jaws will be identified by their orthodontist and referred to see a surgeon to discuss whether surgical correction of the jaw abnormality is an option the patient would consider. Although the jaws may be malpositioned, the orthodontist may be able to obtain a normal occlusion (class I) by extracting teeth and compensating the occlusion. Dental compensation means pulling the upper incisors posteriorly and tipping the lower incisors forward for an overbite. In an underbite, the upper incisors are pushed forward, and the lower incisors pulled posteriorly. Although the occlusion will be excellent there can be some negative sequalae on facial aesthetics which will be discussed by Dr. Baker (see Unintended Consequences of Uncorrected Skeletal Malposition). Nonsurgical jaw growth modification is also an option to correct jaw abnormalities in a growing patient, but if your orthodontist referred you to Dr. Baker, he or she feels you are a potential surgical candidate.
Young professionals are an increasing population of surgical candidates. These are patients who have undergone previous orthodontic therapy in their youth and have either outgrown the correction or are not pleased with the effects of compensatory orthodontics on their facial form. Some of these patients may be able to obtain their desired aesthetic goals through orthognathic camouflage (Make this a clickable link to section Orthognathic Camouflage), meaning procedures on the nose and chin that create the appearance of a normal jaw relationship. Others desire that their problem be addressed by correcting the underlying problem, the jaw malposition. Historically, traditional orthodontic metallic brackets were required before and after surgery, which ended the thought of surgical correction for most patients. With the introduction of clear aligner orthodontics such as Invisalign, metallic braces are no longer required expanding the surgical option for this patient population. This relatively easy process allows young professionals to achieve their desired aesthetic and functional goals with minimal impact on their professional life.
Sleep apnea is a serious disorder that has a negative impact on health similar to smoking tobacco. Uncontrolled obstructive sleep apnea (OSA) can cause pulmonary hypertension, right sided heart failure, as well as daytime drowsiness leading to potential life-threatening accidents. Jaw surgery is NOT a first line approach to OSA. Patients who become candidates for OSA jaw surgery have documented severe sleep apnea on a polysomnogram and have failed more conservative means of therapy such as ENT procedures and CPAP (continuous positive airway pressure).
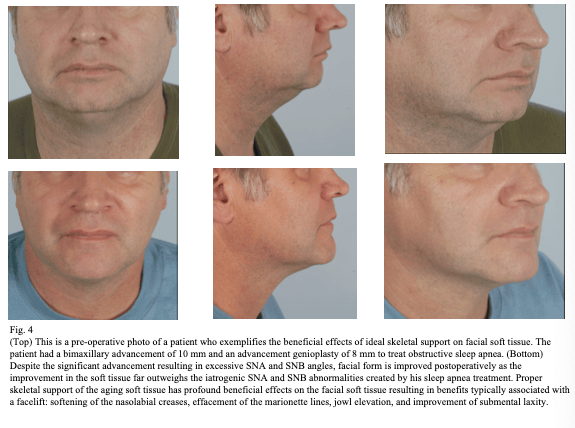
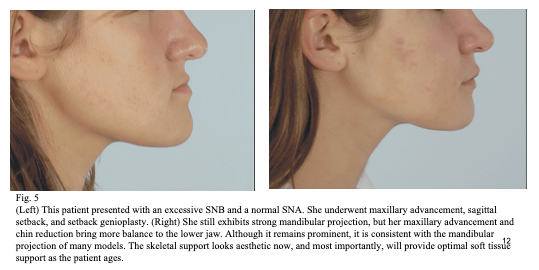
However, for patients who meet the criteria for surgery, two-jaw advancement surgery is very effective at eliminating or significantly improving OSA. Both the upper and lower jaws are moved forward typically at least 10mm which opens the posterior airway and reduces airway resistance.OSA patients frequently inquire if they will look strange having both their jaws moved forward 10mm. Because most OSA patients are middle to older age, the expansion of facial soft tissue that occurs from bringing the bones forward actually has a powerful rejuvenative effect on the facial soft tissue giving almost a facelift effect as the creases and folds soften due to being expanded by the advancement of the jaw bones (see Fig. 4 on page 12).
Facial rejuvenation is a more recent group of patients presenting for orthognathic surgery. With the increase in tele meetings, even before Covid, people realize how they appear on camera and desire improvement. What was surprising to Dr. Baker is that some of these patient’s primary concern were their jowls, submandibular fullness, and marionette lines around the mouth, yet they were presenting for corrective jaw surgery realizing that when their lower jaw and chin were brought forward, their soft tissue appearance greatly improved. In other words, the patient’s motivation for jaw surgery was not to correct the bite but to restore normal skeletal support of the facial soft tissue thereby correcting the soft tissue laxity. This is a very common phenomenon; many of Dr. Baker’s patients seeking face and neck rejuvenation for cosmetic purposes have weak lower jaw and chin projection that significantly contribute to soft tissue laxity and the appearance of a prematurely aged face. In fact, in some of these patients a chin advancement with an osseous genioplasty creates a result that looks superior to that of a neck lift in that there are no visible scars.
Facial asymmetry is an interest of Dr. Baker and in severe cases jaw surgery is necessary to correct the asymmetry with the best result. In almost all cases of facial asymmetry the treatment plan will; include surgery on both the upper and lower jaws as well as the chin. Fat grafting and/or a buccal lipectomy may also be performed to optimize postoperative facial symmetry.
Advances in Current Approaches to Jaw Surgery
New appreciation for adverse aesthetic consequences of untreated jaw discrepancies
- Soft tissue support
- Facial proportion and projection
Clear aligner therapy eliminate the need for traditional braces before and after jaw surgery
Recovery has improved due to advances in technology
- 1 night in hospital
- 2 weeks rubber bands after surgery and then back to clear aligners with no visible braces
- Back to work in as soon as 1-2 weeks after surgery
Clear Aligner Orthodontics (Invisalign)
Clear aligner therapy (CAT) such as Invisalign allows the orthodontist to prepare your teeth for surgery without the need for traditional metal appliances. CAT is an almost invisible way to achieve orthodontic preparation and has lowered the barrier for surgical correction for young professionals who are interested in correcting underlying skeletal jaw discrepancies. Because the teeth do need to be secured during the actual surgery, Dr. Baker will apply temporary fixation devices that are used to apply post-operative rubber elastics for two weeks after surgery.
Definitive Surgical Treatment Plan
The definitive surgical consultation is conducted once the orthodontist and surgeon have finalized a treatment plan. The need for orthodontic preparation before surgery is confirmed. The basic principles of the specific surgical treatment, general sequence of events of the surgical phase of treatment, hospitalization time, time to recover, and the need for a soft food diet are discussed.
Treatment results of patients with similar dentofacial problems may be used to explain the surgical objectives. A patient information brochure is provided and the patient reassured that during the preoperative orthodontic phase, he or she is welcome to discuss with Dr. Baker any concerns regarding the planned surgery. The estimated costs, including costs of the planned surgery, hospitalization costs, and the anesthetization fee, should also be discussed at this stage.
Developing a Treatment Plan
The final pretreatment consultation takes place only after a systematic patient evaluation has been conducted and the orthodontist and surgeon have agreed on a final treatment plan. It is mandatory that the patient (and perhaps the parents or spouse) be well informed. Well informed patients follow instructions and, as a general rule, are easy to treat.
Dr. Baker makes every effort to explain if surgery is necessary, what the advantages and disadvantages are with or without surgery, what is entailed in surgery, and what can be expected during the preoperative and postoperative periods. Risks and complications are also discussed with the patient. He will review specifics of the surgery with plastic models in his office. Finally, a Powerpoint presentation is reviewed that shows typical results as well as a diagrammatic representation of the surgical procedure. Dr. Baker takes pride in informing his patients and gaining their confidence. Dr. Baker will keep explanations simple and to use the your radiographs and dental casts to demonstrate the problems. Solutions for the problems will be discussed in general terms and the need for surgery explained. The importance of preoperative alignment of the teeth and the possibility of the bite not improving or even getting worse during this phase is explained to the patient.
Treatment planning for jaw surgery is a complex process. As Dr. Baker has been practicing over the past 20 years, his approach to treatment planning has evolved. In the most rudimentary sense, the goal of orthognathic surgery is a normal occlusion, but if the jaws are being moved to correct the occlusion, they can be positioned three dimensionally in any desired location while achieving an ideal occlusion. A more sophisticated approach to treatment planning is to think of the surgery as an opportunity to address not only the occlusion but facial shape, skeletal projection and support of the facial soft tissues.
As a dually trained oral & maxillofacial, plastic, and craniofacial surgeon, Dr. Baker has a unique ability to develop a treatment that will be aesthetically pleasing in the present but will also provide the patient with a result that will remain aesthetically optimal as they mature. Dr. Baker has an active practice in facial rejuvenation and has a thorough understanding of the anatomic factors that contribute to facial aging. Rather than relying on traditional cephalometric analysis, Dr. Baker approaches the evaluation of his patient’s face as a plastic surgeon. He observes the support of the soft tissue and evaluates the underlying regional skeletal support and how it is contributing to the overlying soft tissue. In youthful patients these findings are subtle but Dr. Baker’s experience in facial rejuvenation in more mature patients gives him he ability to predict how a young patient will age based on their skeletal proportion and projection. Dr. Baker’s experience in both jaw surgery and facial aesthetic surgery provide him a unique ability to develop a treatment plan that optimizes facial skeletal support creating a result that will delay the effects of gravity and tissue laxity thus prolonging a youthful look as the patient matures.
Once Dr. Baker has completed his physical examination, he will discuss the various approaches to correct your malocclusion. There is almost always more than one acceptable approach and Dr. Baker will discuss the pros and cons of each. In order to help the patient identify which approach they prefer, Dr. Baker will take 3D images and alter them to simulate the expected aesthetic outcome of each approach.
Jaw Misalignment: Should You Consider Surgery?
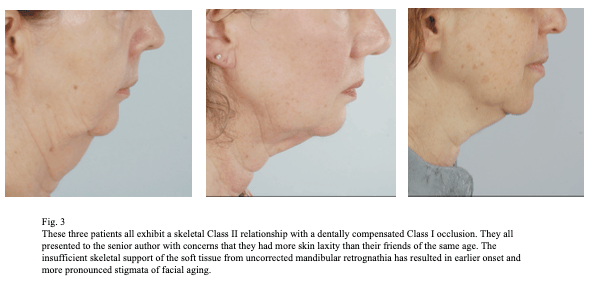
It is not uncommon for the orthodontist to encounter a patient in whom a skeletal discrepancy contributes significantly to dental malocclusion. For many of these patients, the establishment of a normal occlusion can be approached with a surgical orthodontic treatment plan or with dental compensation (correcting an occlusion by extracting teeth or moving teeth without correcting the malposition of the jaw bone/s) alone. Often orthognathic surgery is reserved for patients in whom dental compensation alone would be insufficient. In many cases, an excellent occlusal relationship can be obtained with either approach, but dental compensation alone in a patient with skeletal discrepancy can cause unintended secondary changes that may necessitate future surgical correction. As a plastic and maxillofacial surgeon who performs facial aesthetic surgery, Dr. Baker consistently evaluates patients whose aesthetic concerns are directly related to underlying skeletal deformities that were not addressed when the patient underwent compensatory orthodontic treatment at a younger age. Dr. Baker’s unique training as both an oral & maxillofacial surgeon and a plastic surgeon have provided him the opportunity to observe the unintended adverse aesthetic consequences of dental compensation on facial form in both young as well as mature patients. Dr. Baker has published extensively on this topic and it is his intention that an improved understanding of the aesthetic impact of an uncorrected skeletal discrepancy will aid the patient and the orthodontist in determining the best treatment approach when considering a surgical versus a nonsurgical approach to orthodontic care.
While orthodontists can achieve excellent results in establishing dental Class I occlusion in their patients, they may not be aware of the adverse consequences that compensatory treatment (nonsurgical) may have on facial appearance. As a plastic surgeon with dental training, Dr. Baker has found that a high percentage of his facial aesthetic patients present with aesthetic concerns that are related to underlying skeletal discrepancies of their jaw relationship. Many of these patients have undergone compensatory orthodontics to correct their malocclusion and present with a Class I occlusion. When these patients are informed during their plastic surgery consultation that their uncorrected jaw discrepancy contributes to many of their aesthetic concerns, they frequently report that they were offered orthognathic surgery but did not realize the unintended aesthetic consequences that would result from having a compensatory, non-surgical, treatment approach to their malocclusion.
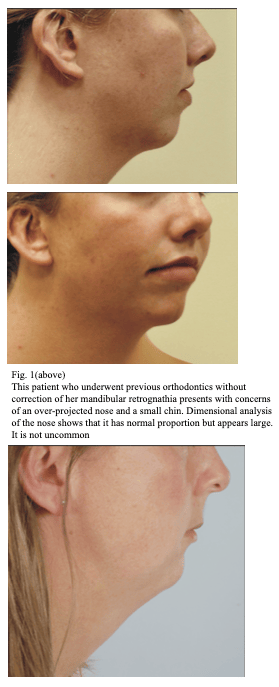 In Dr. Baker’s practice, most rhinoplasty consultations for large or overly- projected noses are in patients with mandibular retrusion and insufficient chin projection. In many cases, the dimensional analysis of nasal form reveals a normal or nearly-normal nasal length and projection that merely appears large due to insufficient lower jaw or chin projection (Fig. 1). When predictive three-dimensional imaging is performed to advance the chin to its ideal position, the nose looks much more balanced with the face and often poses less of a concern to the patient. For this reason, chin augmentation is frequently performed in combination with rhinoplasty in these patients.
In Dr. Baker’s practice, most rhinoplasty consultations for large or overly- projected noses are in patients with mandibular retrusion and insufficient chin projection. In many cases, the dimensional analysis of nasal form reveals a normal or nearly-normal nasal length and projection that merely appears large due to insufficient lower jaw or chin projection (Fig. 1). When predictive three-dimensional imaging is performed to advance the chin to its ideal position, the nose looks much more balanced with the face and often poses less of a concern to the patient. For this reason, chin augmentation is frequently performed in combination with rhinoplasty in these patients.
Almost all patients presenting for chin augmentation exhibit a degree of mandibular retrognathia (retrusion). In patients who were treated with a compensatory approach, it is not possible to advance the mandible to its ideal position to obtain a dental Class I occlusion; thus, increased sagittal projection must be established with chin augmentation. Either alloplastic chin augmentation or an osseous genioplasty can be used to camouflage retrognathia and increase chin projection. Although adolescent patients may not voice concerns over the appearance of a weak chin at the time of initial orthodontic treatment, the aesthetic concerns may become more apparent as the patient enters college or beyond (Fig. 2). Studies have demonstrated a correlation between chin projection and success in the business world for men, and it is important to consider these implications when initiating a treatment plan for the young patient.

Many patients with an underlying skeletal abnormality can obtain a Class I occlusion with dental compensation, but unless skeletal growth modification can restore normal jaw projection, this approach may result in adverse aesthetic consequences that occur long after the patient leaves the orthodontist’s practice. The initial office visit with a patient exhibiting a skeletal abnormality of the jaw should be considered an opportunity for the orthodontist to provide a sophisticated consultation that considers not only the immediate occlusal needs of the patient but also the long-term impact on facial form. It is not the intent of Dr. Baker to imply that every patient with a skeletal discrepancy should receive surgery. It is rather his intention to highlight the importance of education in counseling the patient on the potential benefits and pitfalls of the available treatment options for a dental malocclusion with an underlying skeletal discrepancy, including orthodontic treatment with or without orthognathic surgery for correction of the skeletal discrepancy. It is Dr. Baker’s hope that an improved understanding of the importance of ideal skeletal proportion and soft tissue support will enable the patient and orthodontist to have the information they need to make the best decision regarding their treatment.
Orthognatic Surgical Process
Presurgery
Once a treatment plan has been agreed upon, the presurgical process begins.
Insurance precertification-Please have your orthodontist email Dr. Baker’s office a panographic radiograph, a lateral cephalometric radiograph, a digitized cephalometric analysis and printed models of your teeth. Once we have obtained that information, we will submit to your insurance company for preauthorization.
CT scan-Once we have insurance approval, you will be given a form that specifically indicates the imaging criteria for the CT scan. This can be obtained in a hospital or a cone beam CT scan (CBCT) can be obtained in a dental office. Please keep your mouth closed and teeth together during the imaging process.
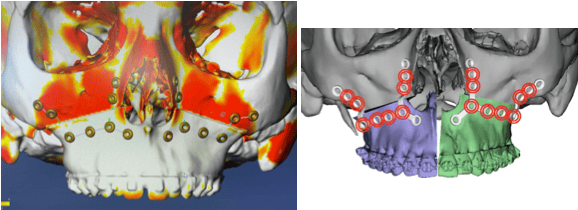
Virtual Surgical Planning (VSP)-Your CT scan will be uploaded to a VSP company to perform your surgery on the CT scan. Splints and custom plates will bedesignedandfabricatedduringthisprocess. Oncethesurgeryiscompleted virtually, splints and plates will be mailed to Dr. Baker for surgery.
Custom plates-Custom plates may be used to precisely place the upper jaw in its desired position independent of the lower jaw, potentially improving the accuracy of the jaw position.
Day of Surgery
The surgery will be performed at Medstar Georgetown University Hospital. The operating room nurses at Georgetown are extremely dedicated to your care. They spend time with Dr. Baker on the weekends doing seminars on optimizing the intraoperative process for jaw surgery cases. The efficiency of these nurses allows Dr. Baker to typically complete a one jaw surgery in 1-2 hours and a two jaw surgery in 2-4 hours. Obviously, surgery is not about speed, but efficiency allows surgery to be performed carefully and smoothly, resulting in a faster recovery for the patient. If you are using clear aligners (Invisalign) instead of traditional braces, Dr. Baker will apply arch bars while you are asleep to serve to rubber band the jaws together in surgery. These are left on for two weeks after surgery and either removed in the OR or the office 2 weeks after surgery.
Recovery
2 Weeks Post Op
3 Weeks Post Op
4 Weeks Post Op
Patients’ perception of the recovery from jaw surgery is almost always much worse than that experienced by Dr. Baker’s patients. Dr. Baker has been at the forefront of incorporating techniques that increase efficiency and expedite recovery in orthognathic surgery. He was one of the first plastic surgeons in the United States to implement virtual surgical; planning into the routine care of orthognathic surgery patients. He is also one of the first surgeons in the United States to perform “splintless” surgery through the use of custom plates. and has presented and published extensively on this subject.
The patient will spend one night in the hospital and usually go home the next day after breakfast or lunch. The jaws are not wired together; elastic rubber bands are used to stabilize the new bite. A full liquid diet is recommended, and the patient should be able to open and close their mouth a little with the elastics in place. A large syringe with a rubber tube attached is used to push fluids into the mouth if drinking is difficult. The first week is tough. Most patients experience swelling, drooling, slight discomfort, and a sluggish feeling. By the second week, patients are able to work on their computers and begin to feel better. After two weeks, most patients start to feel normal. Dr. Baker usually removes his elastics after two weeks, but the orthodontist may require them longer to help guide the new bite. The elastics placed by the orthodontist can be removed and do not restrict opening too much. Numbness starts to resolve but lower lip sensation will return over months. The patient can start on soft solid foods after two weeks and return to a regular diet in 6-8 weeks.
Virtual Orthognatic Surgical Planning
The Team-Medstar Georgetown Nursing

operative assistants they can be. I am so fortunate to work with such dedicated and compassionate team members. They ALWAYS put the patient first!
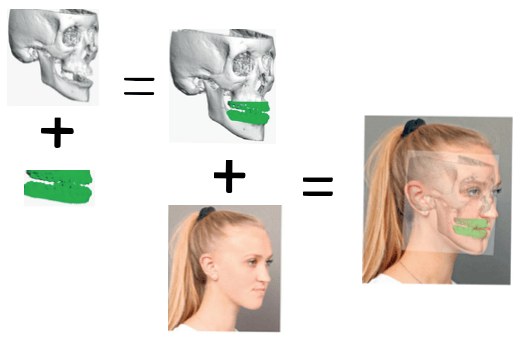
Step 1 After the treatment plan has been established, the patients teeth are scanned to print dental models and a CT scan of the face is obtained. The dental scans are incorporated into the CT image of the patient’s face. A 3D photographic image can be placed over the 3D CT and the data are uploaded to to the virtual surgical planning site
Ancillary Procedures with Orthognathic Surgery
Chin surgery
The chin plays an important role in facial proportion, shape, and soft tissue support. After the jaws have been moved into their desired location, the chin may no longer be in an ideal position in relation to facial proportion. A genioplasty is easily performed at the time of jaw surgery to create the optimal aesthetic result with the same recovery period. There is no functional benefit to the chin surgery, so insurance does not cover the procedure, but Dr. Baker’s office can give you a price estimate. Not everyone is a candidate for a genioplasty when having jaw surgery, but Dr. Baker will inform you if he feels it may be beneficial to your result. He can demonstrate the result with and without the chin to help you make your decision.
Rhinoplasty
The nose plays an important role in facial proportion, shape, and soft tissue support. After the jaws have been moved into their desired location, the preoperative nasal proportion may not be in harmony with the new facial proportion, or more commonly, a pre-existing nasal concern may be more noticeable now that the abnormal jaw relationship has been corrected. Unlike the chin, the nose cannot be operated on at the time of jaw surgery. During jaw surgery, the anesthesiologist’s breathing tube is in the nose preventing Dr. Baker’s ability to perform a rhinoplasty at this time. If the patient desires a rhinoplasty, it would be scheduled at least three months after the jaw surgery.
Liposuction
In middle aged patients, there may be a concern of submental fat under the jaws or chin. This can easily be addressed during jaw surgery with submental liposuction. Liposuction removes excess fatty tissue further defining the jaw and neck postoperatively.
Neck Tightening
If laxity under the chin and neck is of concern to the patient, a mini neck tightening procedure can easily be performed during the jaw surgery. This enhances the result obtained from the jaw surgery. This procedure is typically not desired by patients younger than 40, but for patients who have concerns of their neck, the recovery is combined with the jaw surgery with little, if any additional pain or swelling, making neck tightening an attractive option for some patients.
Lip Lift
The amount of incisal show at rest is a key determinant of vertical maxillary position and facial aesthetics. If a patient does not show a 3-5mms of upper incisors in a relaxed position, the maxilla is planned to be moved inferiorly to obtain the desired degree of incisal show. However, if the degree of inferior positioning required to establish ideal incisal show is excessive, an alternative approach is a lip lift. A lip lift removes upper lip tissue just beneath the nose shortening the length of the upper lip and exposing more visibility of the upper incisors. A lip lift can be performed simultaneous to orthognathic surgery.
Buccal Lipectomy
Dr. Baker is very judicious in selecting patients on whom he performs buccal fat pad removal. A buccal lipectomy is an easy procedure that can be done in the office and typically has a positive aesthetic effect on a young patient. However, having been in practice for over 20 years, Dr. Baker has treated many patients who have had buccal lipectomy in their youth, only to regret it as they age. These patients will present with concerns of facial wasting and cheek hollowing that may be difficult to restore. Fillers are commonly used to treat this problem, but their effects are temporary and expensive to maintain. In select patients who meet his indications, Dr. Baker will perform this procedure, and it may be an enhancing adjunctive procedure in jaw surgery.
Surgical Techniques
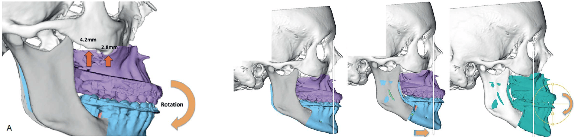
Jaw surgery can broadly be divided into three main procedures: maxillary (upper jaw) surgery, mandibular (lower jaw) surgery, and chin surgery. These structures define facial form in terms of proportion, projection, and soft tissue support. All of these procedures are performed intraorally, thus leaving no visible scars. Once mobilized, the bones can be placed three dimensionally into any position and Dr. Baker’s treatment plan will guide the final postion into the most functional and aesthetic result.
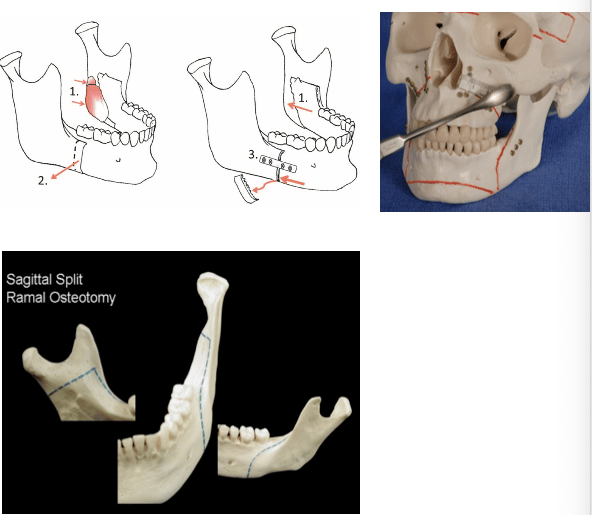
Mandibular (Lower Jaw) Surgery
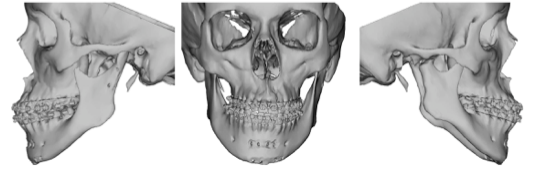
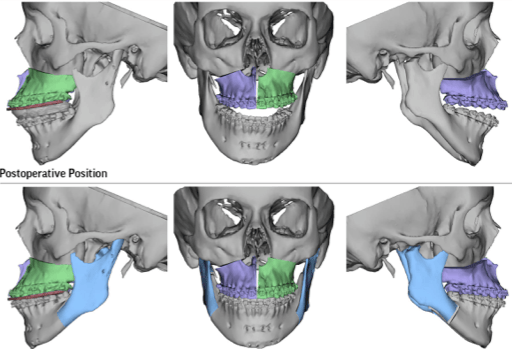
An intraoral incision is used to make a cut in the bone along the red lines of the lower jaw on the model on the lower right. This is also depicted on the diagram on the left. A plate is used to stabilize the lower jaw segments while they heal.
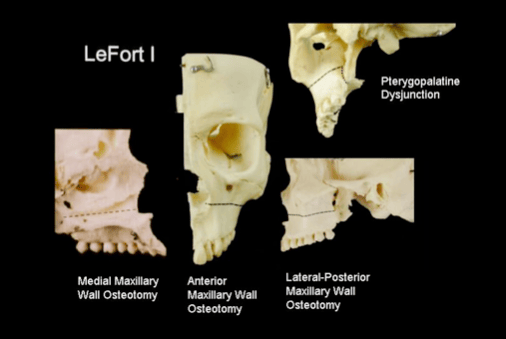
Maxillary (Upper Jaw) Surgery
Orthognatic Surgery Risks and Complications
Sensory nerve damage-Stretching of the infraorbital nerve will cause some temporary numbness in the cheeks and this typically resolves within a few weeks of surgery. The inferior alveolar nerve runs through the lower jaw and will result in some postoperative numbness of the lower lips. About 75% of the time, it will return to normal, about 25% of the time there may be a noticeable, but not bothersome deficit, and approximately 1% of patients may experience bothersome permanent numbness.
Tooth root injury-There is a chance that a tooth root may become injured requiring a root canal.
Infection-Infections are possible with any surgery and may require revision surgery or IV antibiotics.
Bleeding-The need for transfusions is extremely rare but possible.
Nonunion/malunion-The bones my not heal normally requiring secondary surgery to correct.
Plate/screw issues-Occasionally a plate or screw may loosen or become painful. If this happens, removal may be indicated.
Need for revision surgery-Surgical revisions are a potential complication of any surgery.
Undesirable aesthetic consequences– Orthognathic surgery is the most powerful operation to change facial appearance. Almost always the patient is very happy with the aesthetic changes but it is possible, that a patient does not like their new appearance, and a revision may be necessary.
There may be other less common risks and complications that are not mentioned here.
Postoperative Instructions
Medications
You should have received the following prescriptions:
- Peridex rinse-rinse and spit once in the morning and once before bed Medrol (steroid) dose pack-take as directed
- Zofran-take as directed for nausea
- Pain medication-take as directed for pain
- Antibiotics-take as directed
The following “over the counter” medications are recommended
- Saline nasal mist (Ocean Spray)-use to moisten nose as much as desired
- Afrin-TRY TO AVOID. Definitely, do not use more than 3 days duration.
- Pseudoephedrine-take 30mg every 6 hours as needed
Diet
You will be sore after your surgery and limited to a soft diet. High calorie fluids such as Premier Protein shakes, Gatorade protein shakes, Muscle Milk, Ensure, Sustacal, GNC protein shakes, Carnation instant breakfast etc. are recommended for maintaining nutrition. Liquid yogurt such as “Gogurt” and “Danimals” are both easy to ingest and good sources of protein. Also, the “Magic Bullet” blender is a useful item to blend almost any food into a liquid meal. This item can be ordered online. It is not unusual to lose 10-15 pounds after surgery. You should minimize this weight loss by forcing yourself get as many calories as possible. When your body is healing, it requires extra nutrition. Soft foods such as scrambled eggs, yogurt, ice cream, oatmeal, pudding, and soup, are all okay. Initially after surgery, it may be helpful to put the fluids in a 60cc syringe and use a red catheter to feed yourself. The nurses in the hospital will aid you in this technique. Sports bottles with long straws that can be squeezed are good for getting liquids into your mouth easily after surgery. These can be purchased at any sporting goods store and are used for helmet sports such as hockey, football, lacrosse, etc.
Jaw Mobilization
The typical patient does not have his/her jaws wired shut. Usually, rubber bands are used to allow the patient to be guided to his/her new occlusion. These are tight at first and are gradually loosened up to 2 weeks after surgery at which point they are removed.
Nausea and Vomiting
It is not unusual to experience nausea and vomiting postoperatively. Usually, this is limited to the immediate postoperative period and is related to either blood that was swallowed during surgery or the medications that were used in anesthesia. Zofran is one of the medications that you have that will help minimize this problem. If nausea/vomiting persist for more than 3 days, call Dr. Baker’s office.
Bleeding
It is not unusual to have some blood come out of the nose immediately after surgery. If this becomes significantly worse or seems to be actively bleeding, call Dr. Baker’s office immediately.
Pain
Surprisingly, this procedure is not very painful compared to other procedures. The nerves that cause you pain in your cheeks and lower jaw are going to be temporarily numb from the nerve stretching that occurs during this surgery. The prescribed pain medication should be taken as directed for postoperative pain. What does occur is a feeling of malaise and lethargy. This feeling may take several weeks to resolve.
Sutures
All the sutures are dissolvable except the small sutures on each side of the cheek. These are only present if Dr. Baker performed lower jaw surgery. It is normal for the sutures on the inside of the mouth to last about 2-3 weeks before they dissolve.
Oral Hygiene
You may gently brush your teeth with the softest possible toothbrush and toothpaste. Use the Peridex rinse too as this has excellent antibiotic activity. A Water PikTM may be used directly on the teeth and or splints but NOT into the wounds or at the sutures.
Swelling and Bruising
Swelling (edema) will be significant. Jaw surgery is a major procedure that involves mobilizing facial bones. It is totally normal to experience a large degree of swelling. Most of this resolves by 3-4 weeks; however, subtle degrees of improvement will occur for up to a year. Bruising is minor in teens but can be more prominent in adults. It is recommended that you wear the elastic “jaw bra” for 2 weeks 24 hrs/day and then wear it at night only for 4 weeks after surgery.
Numbness
It is normal for both cheeks and lower lips to be numb for up to several months after surgery. This numbness gradually improves with time, and almost all sensation will return to normal with time.
Congestion
Because this surgery involves the maxillary sinuses, you will experience some congestion for several weeks postoperatively. Pseudoephedrine will help this. This is an “over the counter” medication that can be taken as directed. Be careful not to use nasal sprays that constrict the mucosa (Afrin, etc.) for more than 3 days. Prolonged use of these drugs can lead to severe nasal congestion.
Bathing
You can bathe as soon as it is comfortable. Obviously, if you are dizzy or feel faint, do not get into a shower or bathtub and risk a fall. You should have a chaperone until you feel strong and well enough to ambulate and move well without assistance. It is okay to get the face wet in the shower, and baths are okay unless an incision was made on your hip to harvest bone, in which case, you want to avoid water submersion for 14 days.
Orthognatic Surgery FAQs
Contact Information
If you need to contact Dr. Baker’s office use the following numbers as instructed:
8:30am-5:00pm 202-444-7073. After hours call 202-444-7243 and have the plastic surgery resident
on call paged. If you do not receive a response, you should have the page operator page Dr. Baker.
My Surgical Checklist
Orthodontist:
____Radiographs: panorex, lateral cephalometric radiograph ____Digitized cephalometric analysis
____Digitally printed models of upper and lower teeth
All above plus photographs necessary for insurance pre-certification
Dr. Baker’s office:
____2D photographs-facial with lips relaxed and separated and full smile, all facial views and occlusion
____3D Vectra images
____When notified of insurance approval, complete CT scan. An order will be provided along with a specific protocol. Please be sure that the scan is done according to the protocol. If the CT scan was not done at Georgetown, please drop off 2 CDs of the CT scan images at our office in Georgetown or McLean.
As Featured In