Corrective Jaw Surgery & Facial Profiling
Jaw imbalance can affect how your teeth fit, the appearance of your face, and your ability to breathe comfortably. Stephen B. Baker, MD, DDS, FACS, offers corrective jaw surgery and facial profiling for patients who require more than superficial changes. With advanced training in both medicine and dentistry, Dr. Baker addresses jaw structure and facial balance simultaneously, helping you determine whether true orthognathic surgery or a camouflage approach is the most suitable solution.
What Is Jaw Surgery and Facial Profiling?
The spectrum of jaw correction
Jaw concerns exist on a spectrum, ranging from true skeletal imbalance to milder cosmetic disharmony. For patients with significant jaw misalignment affecting bite function or airway health, corrective jaw surgery is considered the gold standard. In other cases, where the skeletal discrepancy is mild or surgery is not appropriate, orthognathic camouflage may offer a reasonable alternative.
The key is to identify whether the concern is structural, aesthetic, or both.
True orthognathic surgery: the gold standard
Orthognathic surgery is corrective jaw surgery that repositions the upper and lower jaws, or both, to correct underlying skeletal imbalances. This approach directly addresses bite problems, jaw position, facial proportions, and, in some patients, airway function.
In selected cases, a surgery-first orthognathic approach may be considered, where jaw correction is performed before extended orthodontic treatment. This approach is evaluated carefully and depends on bite stability, jaw position, and orthodontic coordination.
Common procedures include upper-jaw repositioning (Le Fort I osteotomy), lower-jaw advancement or setback (bilateral sagittal split osteotomy), or a combination of both. These surgeries are planned in coordination with your orthodontist and are designed to correct function first, with facial balance improving as a natural result.
For patients with moderate-to-severe jaw discrepancies, camouflage techniques cannot replace the structural correction achieved by surgery. In these cases, surgery provides the most stable and predictable outcome.
Orthognathic camouflage
Orthognathic camouflage refers to techniques Dr. Baker uses to normalize facial form in patients who would ideally benefit from orthognathic surgery but do not desire, or cannot undergo, jaw surgery to correct their skeletal dysplasia. These techniques are intended for carefully selected patients whose concerns are primarily aesthetic rather than functional.
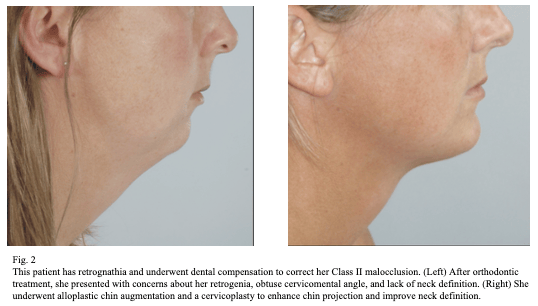
Orthognathic camouflage techniques are also used to address aesthetic concerns in patients who have previously undergone nonsurgical orthodontic treatment despite underlying jaw disharmony. These patients often report being unaware of the facial changes that may result from dental compensation alone. They may later seek to normalize or enhance facial form, proportion, projection, or facial shape.
Patients with an underlying skeletal deformity who undergo nonsurgical dental compensation for correction of their malocclusion may present later in life with aesthetic concerns about their facial appearance directly related to the uncorrected skeletal jaw anomaly. While corrective jaw surgery remains an option, many patients seek alternatives that do not require orthodontic decompensation and bone repositioning.
Orthognathic camouflage and facial profiling
Orthognathic camouflage refers to facial procedures that enhance facial balance without altering the position of the jawbones. This option is considered when the jaw position is only mildly off or when corrective jaw surgery is not the right choice for you.
Many patients seeking camouflage had orthodontic treatment earlier in life that straightened their teeth without changing jaw position. While the bite may function well, the face can still appear unbalanced. Over time, this may show up as a weak chin, a retruded lower face, or a larger nose.
Camouflage focuses on improving the appearance of the face, not the function of the jaws. It does not correct bite alignment or airway concerns and cannot replace true orthognathic surgery when structural correction is needed.
Facial profiling techniques used for camouflage may include genioplasty, chin or facial implants, dermal fillers, fat grafting, rhinoplasty, or surgical lip lifts. These treatments adjust projection and contour to improve proportion while leaving the jawbones in place.
Why camouflage is sometimes chosen
Some orthodontic treatments align the teeth without addressing jaw position. It can correct the bite without changing the underlying jaw imbalance.
When concerns are primarily aesthetic rather than functional, camouflage can help restore facial proportion without the need for jaw surgery. If the discrepancy is more severe, surgical correction should be discussed.
Common camouflage scenario: overbite (small lower jaw)
Patients seeking underbite correction often notice facial imbalance related to limited midface support rather than jaw size alone. A small or underdeveloped lower jaw is one of the most common patterns seen in camouflage patients. In many cases, orthodontic treatment moved the upper teeth backward to align the bite, which can reduce lip support and weaken chin projection.
This combination may make the nose appear larger or the profile less balanced. Many patients seek chin enhancement, facial profiling, or rhinoplasty to improve proportion without jaw surgery.
Often, a large nose is accompanied by a smaller chin. See how balance is addressed on our rhinoplasty page.
Chin enhancement options
Patients often ask about genioplasty vs. chin implant when exploring facial profiling options, as each approach affects projection and long-term support differently. Chin enhancement may be performed using a sliding genioplasty or a chin implant. Genioplasty allows adjustment in multiple directions, improving lower facial support more comprehensively.
Chin implants may be appropriate when forward projection alone is needed. Dr. Baker evaluates facial structure carefully to determine which option provides the most stable balance.
Why structure matters over time
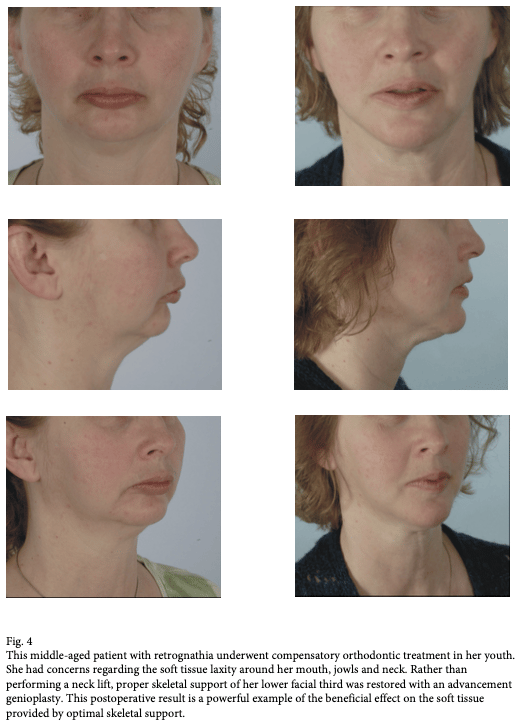
Limited skeletal support can contribute to earlier skin laxity in the lower face and neck. Some patients seek facial or neck procedures sooner due to this imbalance.
In select cases, restoring chin structure later in life can improve soft-tissue support without relying solely on skin-tightening procedures.
Common camouflage scenario: underbite (midface deficiency)
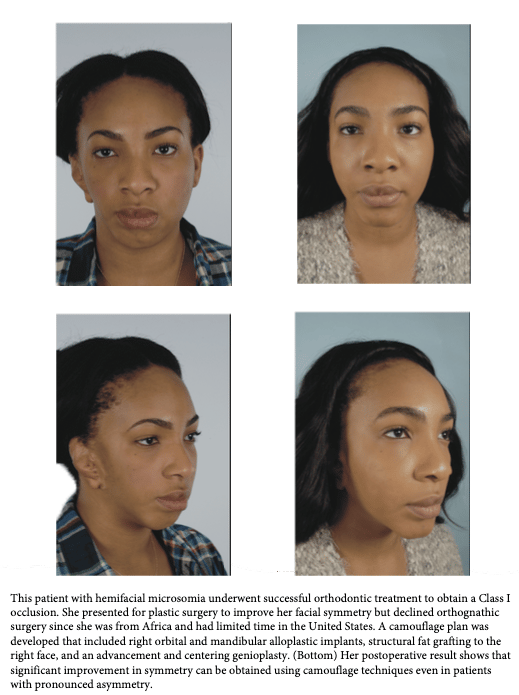
In some patients, the lower jaw appears prominent due to a lack of midface projection. It can affect the area beneath the eyes, the cheeks, and the sides of the nose.
In these cases, camouflage focuses on improving midface and orbital support to soften the appearance of a jaw imbalance.
Advanced facial profiling options
Facial profiling may include implants, dermal fillers, or fat grafting. Implants provide permanent structural support and are often chosen for more pronounced deficiencies.
Dermal fillers enable subtle corrections and allow for reversibility. Technique and placement are selected carefully to maintain smooth contours and natural movement.

What Happens During the Procedure
Corrective jaw surgery is performed in a hospital setting under general anesthesia. Before surgery, detailed imaging, bite analysis, and orthodontic planning are used to map precise jaw movements. This planning guides the repositioning of the upper and lower jaws, or both, to improve bite alignment and facial balance.
During the procedure, controlled bone cuts are made inside the mouth, leaving no visible external scars. The jaws are then carefully moved into their planned positions and secured with small plates and screws designed to remain in place. Surgical time varies depending on whether one or both jaws are treated and the complexity of the correction.
Orthognathic camouflage procedures follow a different approach. These treatments are typically performed on an outpatient basis and focus on facial contour rather than jaw position. Techniques may include chin surgery, implants, or injectable fillers, and they do not involve repositioning the jawbones or altering bite function.

What to Expect During Recovery
Recovery after corrective jaw surgery typically includes a short hospital stay to monitor healing and comfort. Swelling is expected and gradually improves over the following weeks. You will follow a modified diet during the early healing period to protect the jaw position and promote proper bone healing.
Your orthodontist continues working with Dr. Baker as your bite settles into its corrected position. Most patients return to daily activities in stages, with full recovery taking several months as strength and mobility improve.
Camouflage procedures involve less downtime. Recovery depends on the specific technique used, but most patients resume their everyday routines more quickly because the jawbones are not repositioned.
Benefits of Corrective Jaw Surgery & Facial Profiling
Corrective jaw surgery addresses the underlying skeletal structure to improve bite alignment, jaw position, and overall facial balance. Because the correction is structural, the results are stable and designed to last in the long term, while supporting both function and appearance.
Facial profiling enhances facial proportion and projection without changing jaw position. This approach benefits patients with milder concerns who want improved balance but do not require skeletal correction.
How Much Does Corrective Jaw Surgery and Orthognathic Camouflage Cost?
The overall cost of a corrective jaw surgery depends on anesthesia fees, hospital fees, post-surgery garments, medications, and orthodontic coordination. Price is also impacted by medical tests, the surgeon’s fees, and the exact techniques used. Insurance often covers surgery when functional bite or airway issues are documented.
Camouflage procedures are typically elective and paid out of pocket.
Why Choose Dr. Baker for Your Orthognathic Surgery
Stephen B. Baker, MD, DDS, FACS, is one of the few surgeons in the region with advanced training in both medicine and dentistry. This rare dual-degree background allows him to approach orthognathic surgery with a deep understanding of jaw mechanics, bite function, and facial structure. Rather than treating these elements separately, Dr. Baker plans each case as a unified correction of form and function.
As a board-certified plastic surgeon and maxillofacial surgeon, Dr. Baker has extensive experience performing complex corrective jaw procedures, including cases that require close coordination with orthodontic care. His planning process integrates detailed imaging, precise surgical execution, and long-term bite stability, while maintaining careful attention to facial balance and proportion.
Patients choose Dr. Baker for orthognathic surgery in Washington, DC, and McLean, VA, because he offers both true corrective jaw surgery and facial profiling under one practice. This comprehensive approach in our practice supports clear decision-making, coordinated care, and results that address structure, function, and appearance together.
Frequently Asked Questions
Does insurance cover this?
Often, yes, when there is a functional bite or airway issue. Coverage depends on your plan. Camouflage procedures are usually cosmetic and paid out of pocket.
Is facial profiling the same as jaw surgery?
No. Facial profiling enhances appearance without requiring jawbone repositioning. Jaw surgery corrects the underlying skeletal structure.
How long do results last?
Jaw surgery provides long-term structural correction. Camouflage results vary by technique.
Schedule a Consultation
If jaw imbalance or facial proportion concerns are affecting function or appearance, a focused evaluation can clarify your options. Schedule a consultation with Dr. Stephen Baker in Washington, DC, to learn whether corrective jaw surgery or facial profiling is right for you. Contact Stephen B. Baker, MD, DDS, FACS Plastic Surgery to book your appointment.
Related Procedures
As Featured In