Before

After

Before and After Nose Surgery
View Rhinoplasty Before and After Photos
performed by Dr. Baker in Washington DC.
One of the greatest compliments a surgeon receives is the ultimate respect from their peers and the entrusted care of their peer’s loved ones. Dr. Baker is proud of the fact that many of his rhinoplasty referrals come from his colleagues who refer their family and friends to him for rhinoplasty surgery. Every week Dr. Baker sees family, friends, and patients who are referred by fellow plastic surgeons; this is why Dr. Baker is referred to as “The Plastic Surgeon’s Surgeon.”
-Over 20 years of rhinoplasty practice as a faculty plastic surgeon
-Authored textbook on Rhinoplasty
-Authored textbook on Aesthetic Surgery of the Facial Skeleton
-Authored multiple manuscripts on rhinoplasty in peer-reviewed journals
-Rhinoplasty technique instructor at regional national meetings -Awards for best patient outcomes at the Annual Rhinoplasty Meeting
-Visiting Professor on rhinoplasty surgery, American Society of Maxillofacial Surgeons
-Faculty Rhinoplasty live surgery course, American Society of Plastic Surgeons
-Faculty Northeastern Society of Plastic Surgeons Rhinoplasty Symposium
-Member of The Rhinoplasty Society
Professor of Plastic Surgery, Medstar Georgetown University Hospital and Medical School Program Director, Medstar Georgetown University Hospital Plastic Surgery Residency Medical Director, Craniofacial Program Inova Children’s Hospital
Past President, American Society of Craniofacial Surgeons
Past President, Northeastern Society of Plastic Surgeons
Dr. Baker has been a surgical professor in Plastic Surgery at Georgetown University Medical School and the MedStar Georgetown University Plastic Surgery Residency since 2001, and he has trained many of the currently practicing plastic surgeons in the DMV region. Although Dr. Baker has residents and medical students learning from him, they do not perform any aspect of the rhinoplasty surgery. Rhinoplasty is a very precise operation and every step from injecting the local anesthesia to closing the last suture has an impact on the final result. For this reason, Dr. Baker performs every step of the procure himself though he will have residents assisting him in surgery.
While you are evaluated by Dr. Baker for rhinoplasty, he will spend a great deal of time with you to ensure he understands your goals and desires. Predictive 3D imaging is a useful tool to depict various nasal modifications and show you how these will look on your face. It is important that you are an active participant and ask as many questions as necessary to help Dr. Baker determine your goals. It is important to remember that although ideal aesthetic standards of beauty and proportion have been described, each patient has unique goals and desires, and Dr. Baker’s goal is to achieve the nose you desire. If Dr. Baker feels your goals are either inadvisable or unrealistic, he will tell you.
Once you and Dr. Baker have agreed upon the desired result, he will show you the surgical steps that will be performed using his textbook, Rhinoplasty. The book is a surgical atlas with diagrammatic representations of normal anatomy and how each of the many individual maneuvers of rhinoplasty is performed. Before and after images of other patients may also be viewed at the visit. The nose has a central location on the face and plays an important role in one’s perception of facial beauty. Given the importance of rhinoplasty, Dr. Baker recommends at least two visits before surgery to ensure that your questions, concerns, and goals are clarified and answered to your satisfaction before surgery. Before Dr. Baker performs surgery, he requires that the patient can clearly identify their goals, has realistic expectations, and appears well-informed of the procedure as well as its possible risks and complications. In Dr. Baker’s experience, a well-prepared patient will do much better postoperatively leading to a positive experience. In fact, Dr. Baker is well-published in studies evaluating patient-reported outcome measures in rhinoplasty and was awarded the best presentation award at the national Rhinoplasty Society for his work in this area.
Before
After
View Rhinoplasty Before and After Photos
performed by Dr. Baker in Washington DC.
Rhinoplasty is the medical term for a surgical procedure on the nose. Rhinoplasty is performed to help to breathe, improve appearance, or both and is performed in a hospital or outpatient surgery center under general anesthesia.
Primary rhinoplasty is the term used to describe a rhinoplasty on a nose that has not undergone previous surgery.
Revision rhinoplasty is a rhinoplasty that is performed on a nose that has already undergone one or more nasal surgeries. Secondary rhinoplasty refers to a second nasal surgery and tertiary rhinoplasty is done on a nose that has had two previous nasal surgeries. Revision of rhinoplasties may be more difficult due to the scar tissue that is present from previous surgeries. Revision rhinoplasty surgery may require the use of cartilage grafts that are harvested from the nasal septum, ear cartilage, or even
rib cartilage.
Functional rhinoplasty is a nasal surgery that is performed with the sole purpose of improving nasal airflow. Common procedures that have functional benefits are septoplasty, spreader grafts, and turbinate reduction. Minimal, if any, changes in nasal form are seen after a purely functional rhinoplasty.
Reconstructive rhinoplasty is the term used to describe a rhinoplasty that is designed to bring a nose back to its original form after trauma, a congenital anomaly, or a tumor. The patient has a nasal anomaly that requires correction to return to the nose’s normal form. Frequently, both functional and visual improvements are made in a reconstructive rhinoplasty. A reconstructive rhinoplasty does not change the nasal form from the original pre-injury form; its purpose is to return the nose to its original form. A thick nasal tip or dorsal bump that was present before the injury will not be addressed in a purely reconstructive rhinoplasty.

Cosmetic rhinoplasty is designed to change the shape of the patient’s nose to the desired ideal. The patient visualizes their current nasal shape and works with Dr. Baker using 3D images of their nose to define their aesthetic ideal nose. Dr. Baker will help each patient clearly identify their desired changes and make sure the patient has realistic expectations.
It is common to evaluate a patient for a reconstructive or functional problem who is also interested in improving their nasal proportion or appearance. If you are planning on undergoing a functional or reconstructive rhinoplasty and desire additional cosmetic improvement, it is ideal to combine these procedures into one surgery. The recovery is shorter, you save some money on the OR and anesthesia fees, and septal cartilage removed for functional improvement can be used to achieve structural aesthetic improvements reducing the need to harvest cartilage from other sites such as the ear or rib if a cosmetic rhinoplasty is done as a separate surgery.
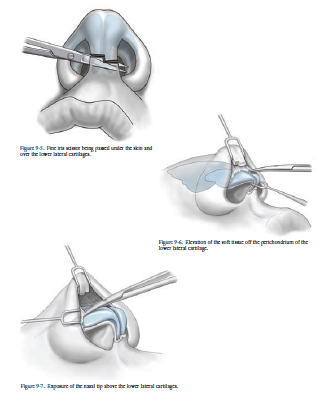
Open rhinoplasty is defined as a rhinoplasty in which an incision is made across the columella to expose the nose. The scar across the columella is so subtle that it can be hard to identify even under direct light and loupe magnification when doing a secondary rhinoplasty. An open approach gives the surgeon much better exposure and accuracy to perform the surgical steps to achieve the final result. It is for this reason that most well-known rhinoplasty surgeons prefer the open technique.
A closed rhinoplasty is performed with all of the incisions on the inside of the nose. This is a good approach for noses that require less sophisticated maneuvers to achieve the patient’s desired result. The limitations of intraoperative visibility make it more difficult to directly and accurately shape the cartilage and place precise positioning sutures. Approximately 25% of the new rhinoplasty patients who see Dr. Baker present for secondary or revision surgery and in Dr. Baker’s experience a high percentage of these patients had their previous surgery through a closed approach.
Non-surgical rhinoplasty is performed by injecting filler into the nose. This may be capable of producing the desired result without the need for surgery by using a dermal filler such as Juvederm or Restylane to create the desired contour. When indicated, it is done in the office with minimal recovery time. A potential complication is that of inadvertently injecting filler into a blood vessel which can lead to tissue necrosis and a wound on the skin of the nose. In rare cases, blindness has even been reported. For these reasons, Dr. Baker recommends that the patient go to a filler injector who also performs surgical rhinoplasties and therefore, has a knowledge of the surgical vascular anatomy of the nose to minimize the risk of the filler is accidentally injected into a nasal blood vessel.
Artificial nasal implants made of Gore-Tex or silicone are easy to place and give a nice immediate result. However, in the nose, they will almost always need to be removed at some point in the future. They can become mobile, infected, or malpositioned. They may extrude through the skin or become encapsulated and look artificial. Most experienced rhinoplasty surgeons do not use artificial implants in rhinoplasty because of their long-term complications. Using the patient’s own cartilage and tissue is the time-tested ideal method to create a durable, safe, and reliable result for the patient. Although more surgical skill is required and the recovery may be longer, a superior result is achieved for the patient.
It looks very natural“Dr. Baker, Thank you for improving my ability to breath and for fixing my nose. Now, when I look in the mirror, I see beyond my nose-I see my face. Immediately, my co-workers complemented me on the skills of my surgeon. Despite the swelling, everyone said it looks very natural and that you have done a good job. Thank you for your skills, understanding, and warm personality. I’m glad I chose you. Thanks!”
Classic ideal proportions of nasal form have been described and are a useful guide for achieving a successful result. However, not every patient desires a nose that fits the criteria for the classic ideal, and typically there is a range of results that are aesthetic but may slightly deviate from the classic “ideal nose.” Using 3D imaging, Dr. Baker will help you determine what nasal changes will result in a nose that you as a patient feel is a beautiful nose.
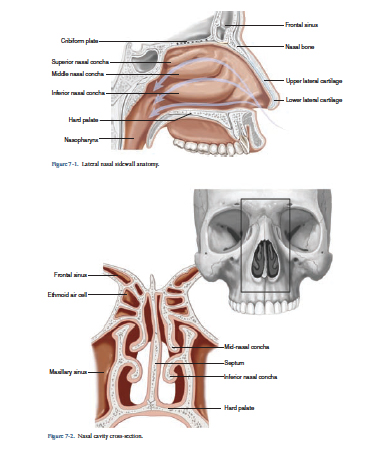
The image below shows the major components of nasal anatomy that are modified in rhinoplasty. The upper portion of the nose is made of nasal bones. The middle third of the nose is comprised of the dorsal nasal septum in the middle and the paired upper lateral cartilages. The lower third of the nose, the nasal tip, is formed from two paired lower lateral cartilages. Finally, the columella, the tissue that divides the nostrils, is made of the medial continuation of the lower lateral cartilages called the medial and middle columellar cartilages.
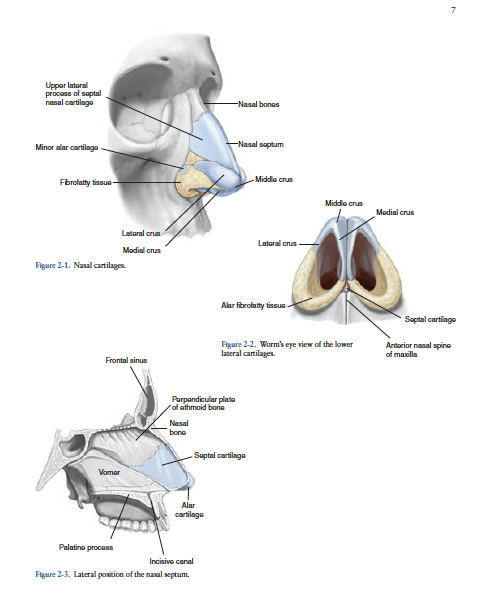
Images courtesy of Rhinoplasty. Taub PJ, Baker SB. McGraw Hill
An elevated dorsum is usually caused by the excessive height of the nasal bones and dorsal septal cartilage. The height of the nose is lowered by incrementally reducing the nasal bones and dorsal septal cartilage to the desired aesthetic ideal. This is usually done using a surgical osteotome combined with the use of a rasp. It is important to realize that after the nose has been lowered, it may appear wider and require other maneuvers to bring its dimension back into proper balance.
A low nasal dorsum can be raised through a variety of techniques. The simplest and that requires the least amount of skill is the use of an implant. There are many reasons this approach is not recommended by Dr. Baker (see introduction page FAQs). Experienced rhinoplasty surgeons almost always prefer the use of autologous tissue (the use of your own bone or cartilage). The preferred technique used by most experienced rhinoplasty surgeons is the use of diced cartilage. This allows a precise elevation and sculpting of the dorsal nasal contour that has a natural feel and appearance. The bone may be used but may resorb and feel stiff. The cartilage necessary is typically harvested from your nasal septum, ear, or rib depending on the amount required to achieve the desired result.
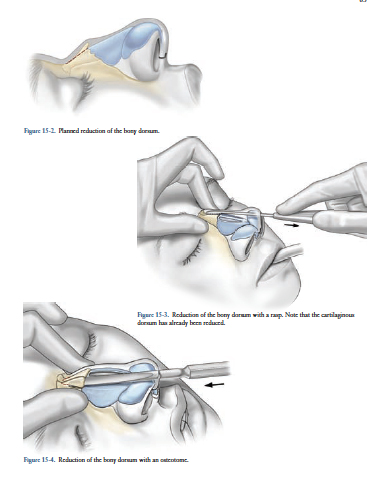
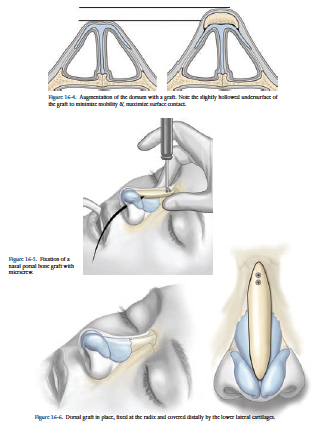
Images courtesy of Rhinoplasty. Taub PJ, Baker SB. McGraw Hill
A bulbous or ill-defined nasal tip is usually the result of broad and large lower lateral cartilages. These are paired cartilage structures that form the nasal tip and contribute to the tip’s definition, symmetry, and size. By removing excess cartilage and using sutures to narrow the tip, Dr. Baker can create a more defined tip. Occasionally, a cartilage graft called a tip graft is added to further define the tip.
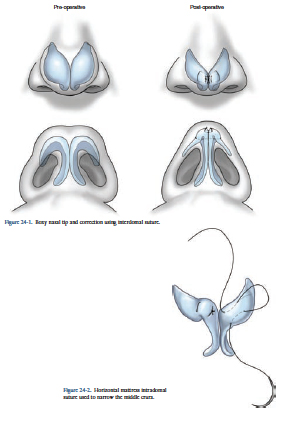

Images courtesy of Rhinoplasty. Taub PJ, Baker SB. McGraw Hill
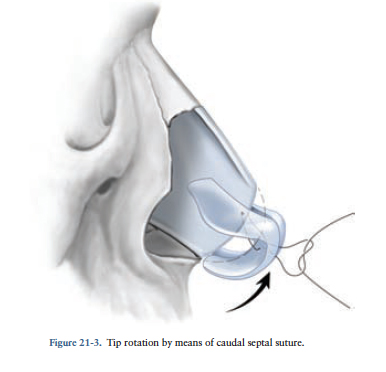
Increasing tip rotation is an easy maneuver that is usually done using sutures to elevate and rotate the tip to the desired position.
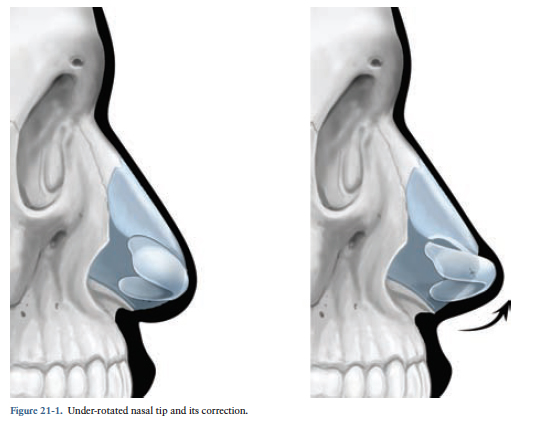
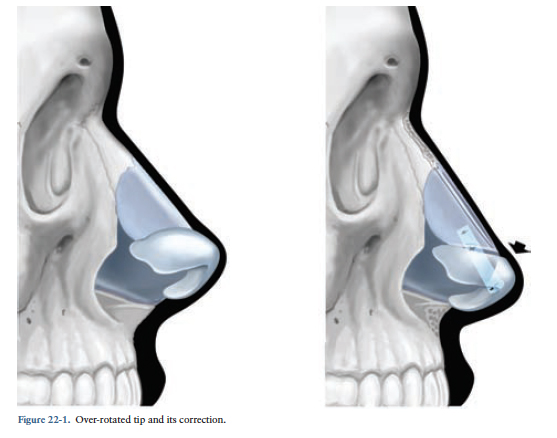
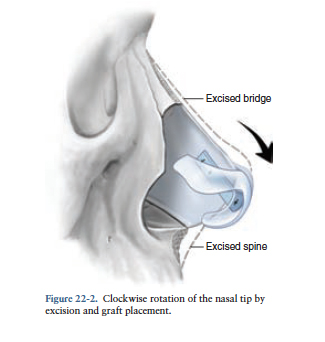
Decreasing tip rotation is usually performed by using a cartilage graft to serve as an anchor to which the tip can be sutured in its desired position.
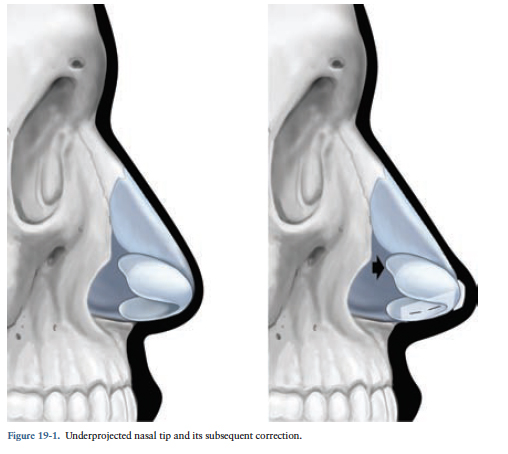
Increasing the projection of the nasal tip is performed through various methods. Sutures may be used to achieve a modest increase in nasal tip projection. Alternatively, a tip cartilage graft may be used to add tip projection and definition. For a more powerful increase in tip projection, cartilage grafts can be used to move the entire tip (both lower lateral cartilages) forward.
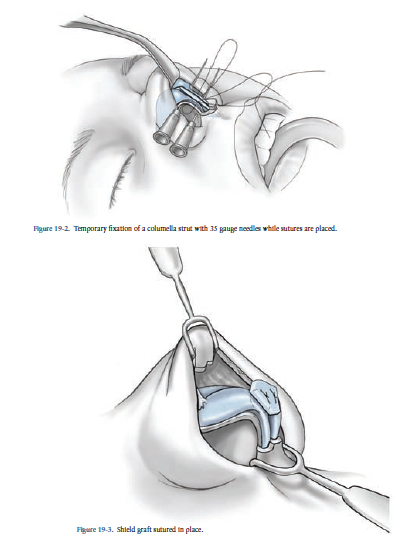
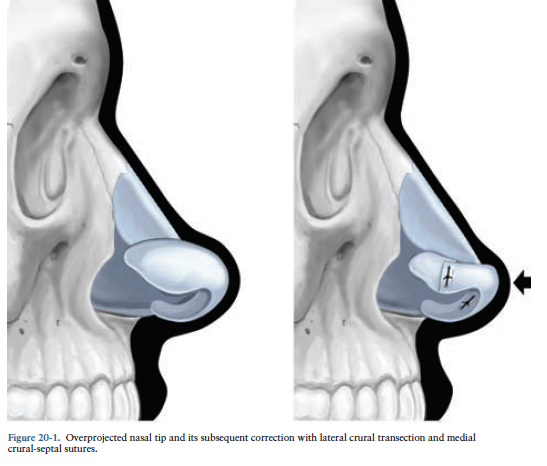
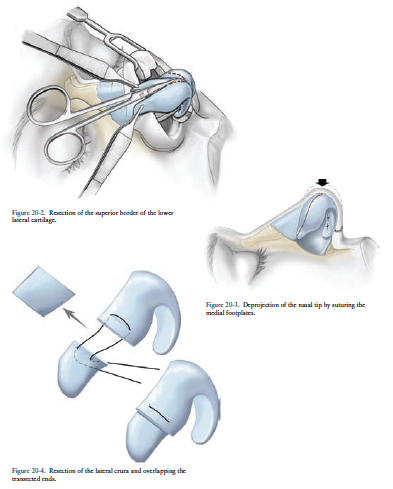
Decreasing excessive nasal tip projection is a challenging maneuver. Because the cartilaginous support is being reduced, there is redundant skin that needs to contract around the new nasal cartilaginous support. For minor decreases in tip projection, the nasal tip can be mobilized and sutured in a more posterior position. Further deprojection can be achieved by removing some of the cartilage in the nasal columella. For the most powerful deprojection, cartilage is removed at the lateral edges and central portion of the lower lateral cartilages, and the tip may be reduced and then covered with a nasal tip graft.
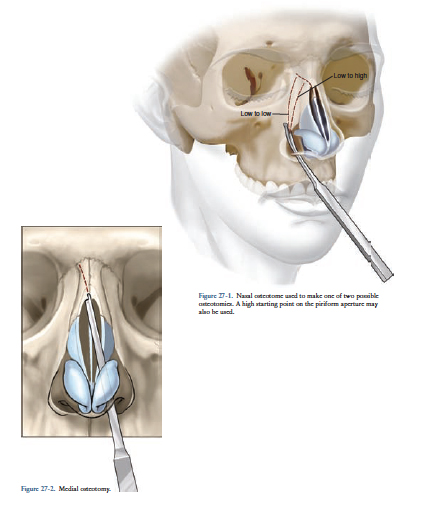
Narrowing the nose is performed in several steps. The tip is narrowed using the techniques described above in Tip Definition. The nasal bones are narrowed by carefully mobilizing the bones allowing them to be moved into the desired position, a procedure known as an osteotomy (see right).
Images courtesy of Rhinoplasty. Taub PJ, Baker SB. McGraw Hill
Correcting nasal asymmetry is a challenging endeavor. Typically, multiple areas of the nose require modification to straighten a crooked nose. The septum usually needs to be corrected with a septoplasty. Occasionally, an intraoral incision must be made to access the septum and center it on the face. The nasal bones frequently need to be mobilized with osteotomies. Tip symmetry is usually corrected with sutures but may require a cartilage graft. Other cartilage grafts are frequently used to reinforce the structure to maintain symmetry and control external forces on the nose.
A breathing assessment is made by direct visual inspection and a test called a Cottle maneuver. If a deviated septum or internal nasal valve collapse is present, spreader grafts or a septoplasty may be indicated. A Cottle maneuver is performed when Dr. Baker occludes one nasal passage and has you breathe through your nose. If breathing is easier when he lateralizes your nostril, it is a sign that you have a narrowing of your internal nasal valves. The internal nasal valve angle is the angle between your septum and the lateral nasal wall. Opening this angle with the Cottle maneuver simulates an adhesive nasal breathing strip that opens the airway. A deviated septum is seen on direct visual examination and can also be evaluated with a CT scan.
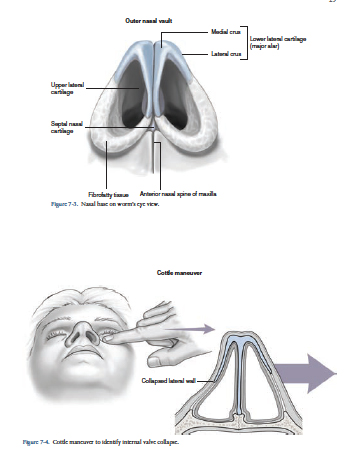
Images courtesy of Rhinoplasty. Taub PJ, Baker SB. McGraw Hill
A septoplasty is performed to remove a deviated portion of the nasal septum that is contributing to nasal breathing problems. Enough remaining septum is left so the nose does not change shape. Additionally, mucosa (skin on either side of the septum) remains after the cartilage has been removed so there is not a hole between the two sides of the nose (lower left).
Using septal cartilage or other cartilage, grafts are placed to open the internal nasal valve angle to help to breathe. When a change in nasal shape is not desired, they are placed in a location that helps to breathe but does not change nasal appearance. However, they can be strategically placed to help with nasal symmetry and structural support if necessary (lower right).
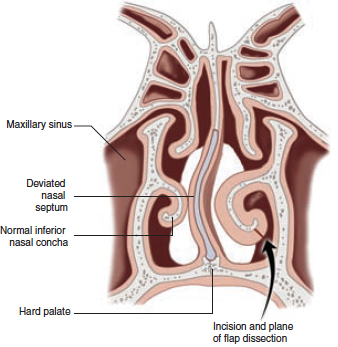
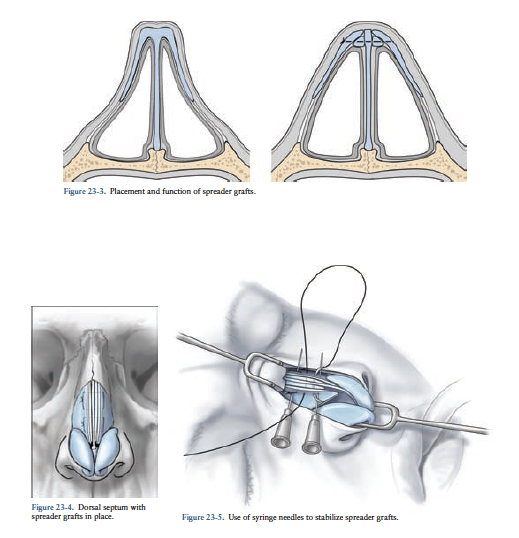
Images courtesy of Rhinoplasty. Taub PJ, Baker SB. McGraw Hill
The turbinates are paired structures located inside the nose. When they are enlarged, they can contribute to airway obstruction. Selective trimming, out fracturing, or reduction can help improve nasal breathing.
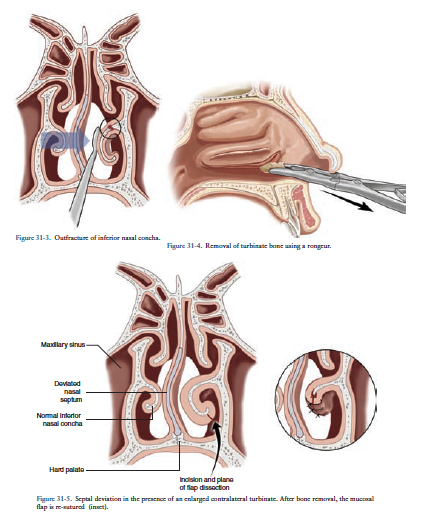
Images courtesy of Rhinoplasty. Taub PJ, Baker SB. McGraw Hill
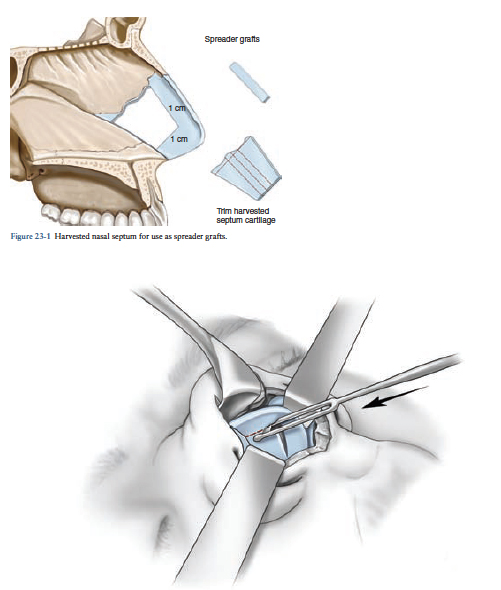
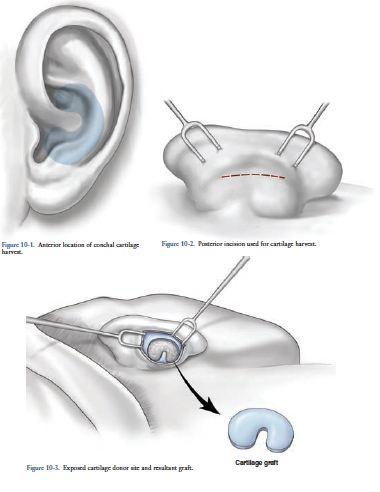
Septal cartilage is the best source of cartilage for use in rhinoplasty. It is flat, strong, and resists warping. Unfortunately, it is limited in supply. Septal cartilage is taken from inside the nose so there is no visible scar (for technique, see septoplasty above).
Ear cartilage is more abundant but is softer and does not provide sufficient rigidity for certain techniques (upper right). Ear cartilage is taken from an incision behind the ear, so this method is very inconspicuous and the shape of the ear does not change. For one week after the harvest, a cushion dressing is applied to keep the skin compressed. The dressing is removed after one week.
Rib cartilage is rigid and abundant but is prone to warping. The rib is accessed through a small 3cm incision in the inframammary fold. It is visible but is small and typically heals well as the scar matures (see the following page).
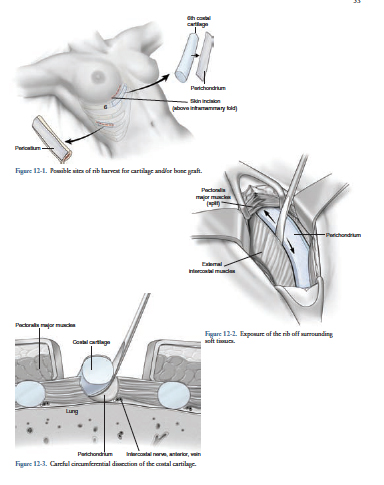
Images courtesy of Rhinoplasty. Taub PJ, Baker SB. McGraw Hill
Please call 202-444-7073 to schedule your post-operative appointment or if you have questions during office hours (8:30-5:00) .
Call 202-444-7243 and ask for the Plastic Surgery Resident on call.
You may shower 24 hours after surgery unless otherwise directed. In the meantime, please sponge bathe as it is important to maintain good hygiene. All dressing should be left in place unless otherwise directed, as they will be removed at your first post-op appointment. It is normal to have drainage from your nose which may be tinged with blood. Usually, the drainage decreases significantly after 36 hours and becomes clearer. You can keep your nostrils clean and free of drainage using Q-tips dipped in hydrogen peroxide but only reach inside the nose as far as the cotton end of the Q-tip.
Depending on the specific nasal surgery you had done, you may have been given a medication for swelling called a Medrol dose pack. The directions for this medication are printed directly on the foil pack and should be followed exactly as printed. The medication should not be stopped abruptly. You should expect to have more swelling and bruising the morning following surgery as swelling will peak 24-48 hours after the procedure. If you can comfortably sleep propped up on pillows this may help to reduce the swelling. If you wear glasses, you may tape them to your forehead with a small loop of tape passed over the nosepiece. When you first begin to wear your glasses, you may notice indentations where they touch your nose. These indentations are not harmful and they will decrease as the swelling of your nose decreases. Almost all of the noticeable swelling should be gone 2-3 weeks after surgery but the thicker areas such as the nasal tip will continue to improve in the definition for several months. Remember that the degree of swelling may be different on each side of the nose even if the same procedure was performed. Don’t worry about these differences for the first 3 weeks after surgery. Improvement in airflow through the nose may not be noticeable until the swelling decreases 2-3 weeks after surgery. The tip of your nose will be quite numb for the first several weeks after surgery. This is normal and as the skin nerves regenerate your sensation should return. Return to normal sensation could take several months.
You have been prescribed narcotic pain medication. Narcotic pain medications can cause constipation. You may find it helpful to take an over-the-counter stool softener while you are taking the pain medication. It is not unusual to have nausea after surgery. You have been prescribed Zofran which can be taken for nausea. You received IV antibiotics during surgery. You may have also been sent home with a prescription for an antibiotic. If you were given an antibiotic prescription, it is important to complete the entire course. You may have also been given a medication for swelling called a Medrol dose pack. The directions for this medication are printed directly on the foil pack. Try to avoid nasal sprays such as Afrin or other types of antihistamine nasal sprays.
Diet restrictions will be specified prior to leaving the hospital as certain procedures necessitate you to maintain a soft or liquid diet for a period of time after surgery. Your throat may be sore following general anesthesia. You may try over-the-counter throat lozenges. No alcoholic beverages while taking pain medication. We recommend a high-fiber diet and lots of liquids while taking pain medication in order to prevent constipation. You may also want to take an over-the-counter stool softener such as Pericolace while taking pain medication.
You will be drowsy after your surgery but this should begin to wear off overnight and into the next day. It is important to begin to resume normal light activity as tolerated. Your energy will return more quickly if you begin to resume normal activity the day after surgery. You should do no heavy lifting (greater than 10 pounds) and no strenuous (activity that raises your blood pressure) activity for 2-4 weeks. Facial surgery patients should avoid contact sports for 8 weeks after surgery. During this time, strong blowing of the nose could disrupt the contoured nasal bone and septum as well as cause significant bleeding. We will specify permissible activity levels as you proceed through your post-operative course.
You should not drive while taking pain medication. If your nose begins to bleed at any time, try to relax and lie down with your head slightly elevated. Use a moist washcloth and apply gentle pressure to the nostril area for 15-20 minutes. If this does not work, call the office if it is during normal business hours. If it is after hours and you can’t get your nose to stop bleeding you should go to the Emergency Room.
A temperature of 101.5 or above
Excessive drainage and/or bleeding
Increased redness
Increased swelling or abnormal swelling of one side compared to the other Pain that is not tolerable after taking pain medication
Inability to urinate within 6 hours of leaving the hospital
The following document is an informed consent form that has been prepared to help Dr. Baker inform you about the nature, benefits, risks, and alternatives to rhinoplasty surgery. It is important that you read this information carefully and completely.
Rhinoplasty surgery is designed and performed to reshape or improve the function of the nose. The techniques utilized may produce changes in the appearance, structure, and function of the nose. They may reduce or increase the size of the nose or change the shape of the various components of the nose, including—but not limited to—the dorsum, tip, and nostrils. They may also change the relationship of the nose to surrounding structures, including—but not limited to—the cheeks, the eyes, and the upper lip. Rhinoplasty may be indicated to correct congenital birth defects, acquired deformities, traumatic injuries, and/or functional problems with breathing. The techniques of rhinoplasty are customized for each patient and are not identical in all patients. The techniques may be performed using either incisions outside the nose or inside the nose or a combination of the two. Patients interested in undergoing a rhinoplasty procedure should have realistic expectations and not expect perfection. They should also be in good physical and emotional health. Rhinoplasty can be performed in conjunction with other surgeries.
With any type of surgery, there is inherent risk. It is always an option not to undergo rhinoplasty surgery. An individual’s choice to undergo any particular surgical procedure is based on the comparison of the risks and potential benefits. Although the majority of patients do not experience these complications, you should discuss each of them with Dr. Baker to make sure you understand the risks, potential complications, and consequences of rhinoplasty. Infrequently, it is necessary to perform additional surgery to improve your result.
Bleeding — It is possible, though unusual, that you may have a problem with bleeding during or after surgery. Should postoperative bleeding occur, it may require emergency treatment to stop the bleeding or require a blood transfusion. Do not take any aspirin or anti-inflammatory medications for 2 weeks before surgery, as this contributes to a greater risk of bleeding. Hypertension (high blood pressure) that is not under good medical control may cause bleeding during or after surgery. Accumulations of blood under the skin may delay healing and cause scarring.
Infection — Infection following rhinoplasty is rare. Management usually involves a course of antibiotic therapy but may also necessitate a return to the operating room for irrigation and/or debridement of infected tissue.
Scarring — Although good wound healing after a surgical procedure is expected, abnormal scars may occur both within the skin and the deeper tissues. Scars may be unattractive and of a different color than the surrounding skin. There is the possibility of visible marks from sutures. Additional treatments including surgery may be needed to treat scarring.
Damage to deeper structures — Deeper structures such as nerves, tear ducts, blood vessels, and muscles may be damaged during the course of surgery. The potential for this to occur varies with the type of rhinoplasty procedure performed. Injury to deeper structures may be temporary or permanent.
Nasal septal perforation — There is the possibility that surgery will cause a hole in the nasal septum to develop. This occurrence is rare. However, if it occurs, additional surgical treatment may be necessary to repair the hole in the nasal septum. In some cases, it may be impossible to correct this complication.
Unsatisfactory result — There is the possibility of an unsatisfactory result from the rhinoplasty surgery. The surgery may result in unacceptable visible or tactile deformities, loss of function, or structural malposition. You may be disappointed that the results of rhinoplasty surgery do not meet your expectations. Additional surgery may be necessary should the desired result of rhinoplasty not persist after surgery.
Numbness — There is the potential for permanent numbness within the nasal skin after rhinoplasty. The occurrence of this is not predictable. Diminished (or loss of) skin sensation in the nasal area may not totally resolve after rhinoplasty.
Asymmetry — The human face is normally asymmetrical. There can be a variation from one side to the other in the results obtained from a rhinoplasty procedure.
Long-term effects — Subsequent alterations in nasal appearance may occur as the result of aging, sun exposure, or other circumstances not related to rhinoplasty surgery. Future surgery or other treatments may be necessary to maintain the results of a rhinoplasty operation.
Nasal airway alteration — Changes may occur after a rhinoplasty or septoplasty operation that may interfere with the normal passage of air through the nose.
Surgical anesthesia—Both local and general anesthesia involve risk. There is the possibility of complications, injury, and even death from all forms of surgical anesthesia or sedation.
Deep Venous Thrombosis and Pulmonary Complications: Surgery, especially longer procedures, may be associated with the formation of blood clots in the venous system. Complications may occur secondarily if blood clots (pulmonary emboli), or fat deposits (fat emboli), travel to the lungs. Pulmonary and fat emboli can be life-threatening or fatal in some circumstances. Air travel, inactivity, and other conditions may increase the incidence of blood clots traveling to the lungs causing a major blood clot that may result in death. It is important to discuss with your plastic surgeon any past history of blood clots or swollen legs that may contribute to this condition.
Smoking, Second-Hand Smoke Exposure, Nicotine Products (Patch, Gum, Nasal Spray): Patients who are currently smoking, use tobacco products, or nicotine products (patch, gum, or nasal spray) are at a greater risk for significant surgical complications of skin necrosis, delayed healing, and additional scarring. Individuals exposed to second-hand smoke are also at potential risk for similar complications attributable to nicotine exposure. Additionally, smoking may have a significant negative effect on anesthesia and recovery from anesthesia, with coughing and possibly increased bleeding. It is important to refrain from smoking at least 6 weeks before surgery and until your physician states, it is safe to return if desired.
Information Specific to Female Patients: It is important to inform your plastic surgeon if you use birth control pills or estrogen replacement, or if you believe you may be pregnant. Many medications including antibiotics may neutralize the preventive effect of birth control pills, allowing for conception and pregnancy.

Rhinoplasty is a cosmetic procedure that is fully customized to address the needs of each individual patient. The cost of this plastic surgery depends on the specific technique used, the degree of correction desired, and the overall complexity required. We will perform an analysis of your nose with respect to your other facial features to develop a surgical plan and discuss the associated cost during your consultation.
Most insurance companies exclude coverage for cosmetic surgical operations or any complications that might occur from cosmetic surgery. If the procedure corrects a breathing problem or marked deformity after a nasal fracture, a portion may be covered. Please carefully review your health insurance subscriber policy.
All instructions given by Dr. Baker should be carefully followed to maximize the success of your outcome. It is important that the surgical incisions are not subjected to excessive force, swelling, abrasion, or motion during the time of healing. Physical activity needs to be restricted. Surgery involves clotting of blood vessels and increased activity of any kind may open these vessels, leading to bleeding, or hematoma. Increased activity that raises your pulse or heart rate may cause additional bruising, swelling, and the need for a return to surgery and control of bleeding. It is wise to refrain from physical exertion (including sexual activity) until Dr. Baker determines it is safe. Protective dressings and drains should not be removed unless instructed by your plastic surgeon. Successful postoperative function depends on both surgery and subsequent care. It is important that you participate in follow-up care, return for aftercare, and promote your recovery after surgery.
If you’re interested in learning more about rhinoplasty in Washington DC, contact our office to schedule your informative consultation today. Our skilled team will help guide you throughout the entire surgical process and answer any of the questions you have along the way.
Wrinkles and fine lines are two of the most common signs of facial aging and ... Everyone dreads the fact that one day they will have to wake up and find ... Sagging breasts, asymmetric breasts, and nipples pointing downwards are common problems that can occur after ...

